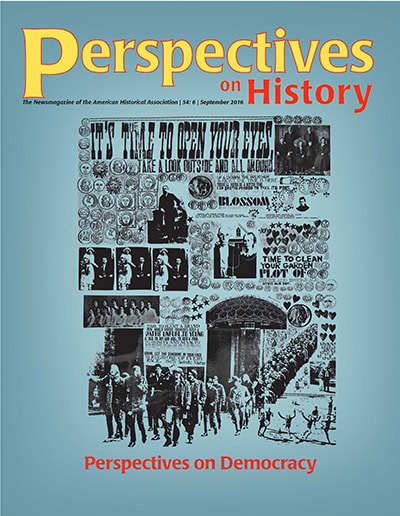
Perspectives on Democracy
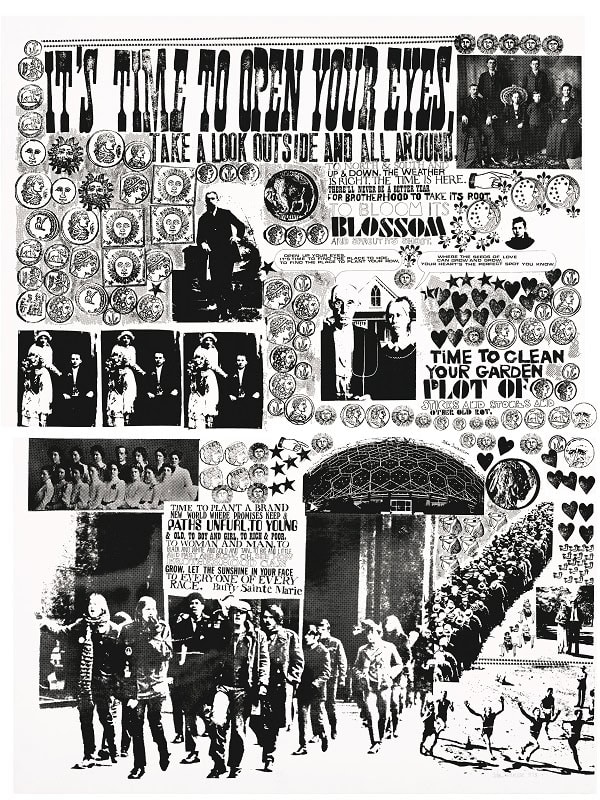
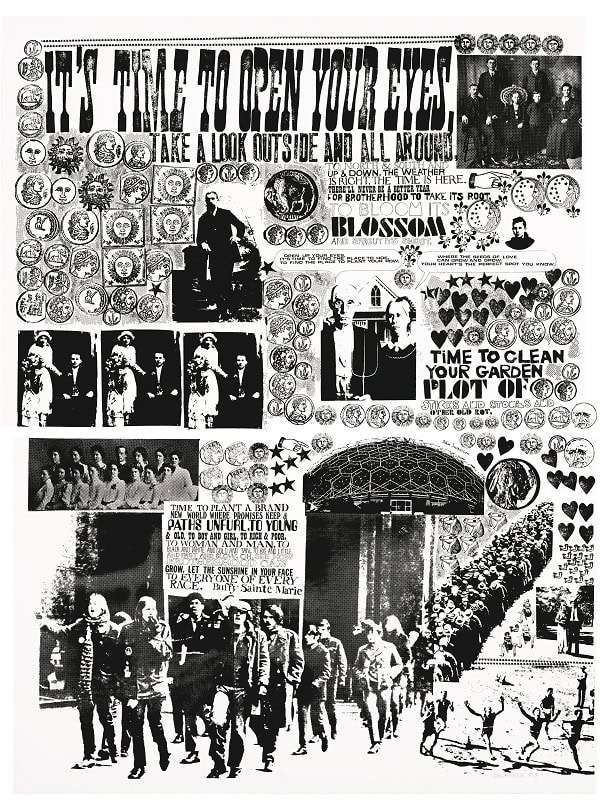
Inspired by the social movements of the late 1960s and early 1970s, Los Angeles artist John August Swanson created a series of collages, reproduced as seriographs, that he called “exploding newspapers.” These combined overexposed photographs, lettering, stamps, and words that were meaningful to him. Seeds of Brotherhood (1973), reproduced on our cover, is one “exploding newspaper” that seems to capture the essence of democracy for us: optimistic, with an underlying order that belies its first impression, and full of people. John August Swanson, Seeds of Brotherhood. Copyright 1973 by John August Swanson. Serigraph, 17.5″ x 23″. www.JohnAugustSwanson.com.
Staff