When Disaster Strikes
We had been planning a themed Perspectives issue on disaster for months. Then the COVID-19 pandemic arrived, making the May issue—the first ever created by an AHA staff working from home—even more relevant. The issue features articles from Jessica Unger on cultural heritage, Laura Ansley on oral history, and R. E. Fulton on the Anthropocene. Nancy Tomes provides context for the Medicare for All debates of the last year, now even more charged in a nation struggling to “flatten the curve” of infection. Finally, executive director James Grossman reports on the AHA’s efforts to support historians during the crisis and president Mary Lindemann gives a medical historian’s view of the pandemic.
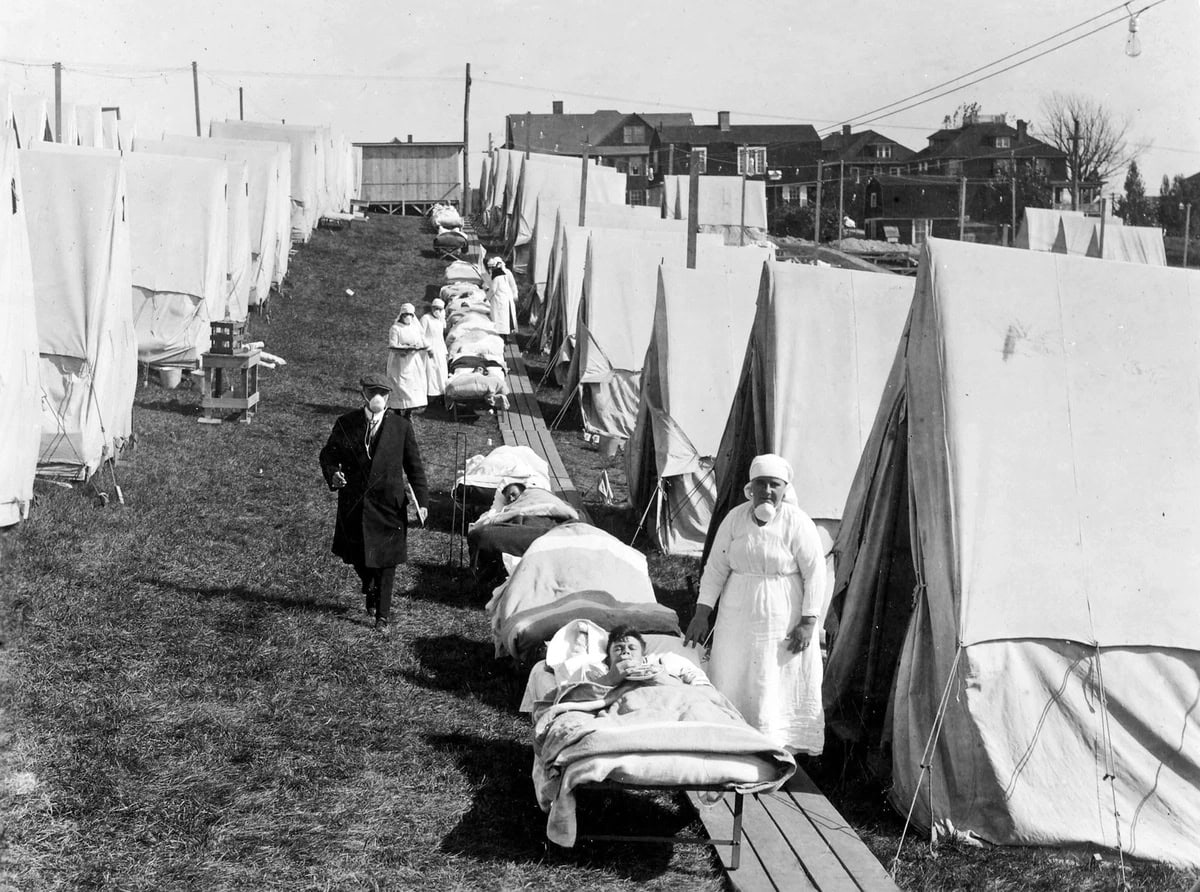
Photo: National Archives and Records Administration, 165-WW-269B-019
Staff











-scaled.jpg)



